


Post-vaccination vs post covid myo/pericarditis in adolescents and young adults: Why & how the CDC just keeps getting it wrong

The employees of the CDC, along with the CDC director, work for all of us Americans. Our tax dollars pay their salary. If they are being paid to simply recite and publish government propaganda or preferentially publish or focus on only the most politically convenient findings, we should be aware of this. And it’s not just a matter of how our money is spent, but of how trustworthy the supposedly scientific information is that comes from our national public health agency.
Perhaps the biggest lesson I learned during the COVID-19 pandemic is if citizen scientists do not step up to do the work, the CDC will continue to mislead the public or simply push policy without doing the studies. I first learned this in 2020 when I was senior author on the Wood County Wisconsin study published in MMWR, which ended up in the top 1% of all scientific papers published during the Covid years. We knew from European (1,2) data already in June of 2020 that reopening schools was not associated with increase community spread, so why was the CDC using COVID-19 test positivity metrics to determine whether or not schools could open when we didn’t have evidence closing them would reduce disease transmission in the first place (And actually had good evidence to the contrary)? If you were following me on Facebook in the spring and summer of 2020, you know how obsessively I was promoting school reopening based on Europe’s experience (we even got the diocese I was medical advisor for open full time that summer in part using the data I had collected and approaches from Scandinavia).
When our Wisconsin study, as expected and like reported from Norway and North Carolina, found such low transmission rates in K-12 schools, it became clear why closing schools never made sense from an epidemiological standpoint. The collateral damage that would ensue from the closures was unquestionable - but a question that did remain was: why did our (unpaid) research group do the work the CDC should have done? And, moreover, why did we have to continue to fight them when they doubled down on needing “metrics” for school closures? I will sound like a broken record to people who know me well, but it bears repeating, you should not have “metrics” for interventions that don’t work and just cause harm. You should just drop them and preferably never start them…
After we published our study (which required a ton of work), I wanted to go back to my old carefree life of working in clinic, hanging with my family and running in the mountains, but I gained an enormous sense of responsibility whether or not I wanted it. After school closures, the biggest issue that worried me was youth sports closures, which I also published on with Alli Krug in the British Journal of Sports Medicine. It’s hard to convey how much needless keeping children out of sports broke my heart- and I had this sense I was in a position to fight it, but how? Meanwhile the CDC persisted in showing they weren’t doing the work we were all counting on (and of course paying) them to do. It’s crazy how out of touch they were to recommend children wear masks outside while playing things like soccer… if the kids were even allowed to play in the first place.
In the winter and early spring of 2021, the CDC started ignoring reports from Israel, including 2 deaths from myocarditis, and 14 cases in their own Department of Defense about vaccine associated myocarditis in young adults. I had the sense in my bones once again the CDC would fail us when it came to a good risk-benefit analysis of the vaccine in adolescents. Of course the rest is history, but it’s not because it’s still happening!
What was clear was citizen scientists needed to step up and do reliable research. But who? (imagine me looking left and right and seeing no one…) Again there was no funding or incentives for this type of research (and we had no idea the attacks that were coming)…but John Mandrola, Alli Krug and Josh Stephenson joined me and we published the first study to suggest for healthy males ages 12-17 the second dose of the Pfizer vaccine carried a higher risk of associated myocarditis than their chance of COVID-19 hospitalization over the next 120 days when incidental hospitalizations were removed. This has been validated now over and over, and eventually published in the peer reviewed journal EJCI. But when we submitted it to MMWR initially in August of 2021, they said our paper did not present “anything that was not already relayed.” (of course except that we found the second dose of the vaccine unfavorable in a large demographic of adolescents!).

CDC eventually acknowledged in Lancet Child & Adolescent Health the harms of myocarditis were worse than they had expected and that of course the safety signal was real. Prospective data (active surveillance) from Hong Kong put the risk at 1/2700 dose 2 Pfizer vaccines in 13-18 year old males, all of whom were hospitalized. This was over twice as high as we had estimated from VAERS in our preprint.
When it comes to masks, CDC, has also proven themselves untrustworthy. They promoted school mask mandates in the absence of high quality data. My own research group (again, unfunded) found no difference in case rates in adjacent school districts in Fargo North Dakota either when they had differing mask policies or the same masking policies (submitting this to a peer reviewed journal is one of the many things on my to-do list!). Meanwhile CDC ignored existing randomized data finding no evidence of benefit (see 2 cochrane reviews) and published what essentially boils down to mask propaganda without a single one of their 77 studies we identified pertaining to masks finding causal evidence that “masks work" in non mannequin humans, yet they claimed masks were causal in reducing cases.
So in our most recent analysis, we wanted to show once and for all, at least when it came to the topic of masks, MMWR was more about the message (“masks work”) than the science of public health (“what evidence do we have masks do or don’t reduce illness?”). But 75% of their published 77 studies pertaining to masks still said masks even though only 30% actually studied masks and yet only 30% studied masks & 0% found causal evidence of effectiveness. Of the 5% that reported higher case rates in the masked group than the comparator group, all concluded masks were effectives! You can’t make this up. It is so bad.

As an aside, I am very proud our research group just had this published in the American Journal of Medicine, after acceptance without revision requests! (It’s an amazing privilege to work with researchers like Vinay Prasad and Alyson Haslam. I think we do important work, but I digress). If you can’t access the full text, see the preprint here, which with the exception of the reformatted abstract should be word for word the same.
Post-vaccination vs post-Covid myo/pericarditis
So are we to believe the CDC Director is correct when she states “teen boys have been up to 5x as likely to get heart inflammation after getting infected than getting vaccinated”?

As far as I can tell, she is citing this study published in MMWR.

But this study has got serious problems:
-In their calculation of how often children get myocarditis after COVID-19, the only children they consider to have been infected were those who sought medical care and their positive covid test was recorded in the EMR (ie had a diagnosis of COVID-19 in the electronic medical record). This drastically and inappropriately shrinks the denominator of # of children infected, overestimating the rate of post-covid myo/pericarditis. (As an example, I imagine my kids have had covid. I have no idea but it’s certainly not recorded in an EMR. They did not get vaccinated; we’re not testing that one out…)
-Sampling bias: of the kids who seek care related to their covid positive test, they will tend to be kids with underlying health problems, maybe even cardiac problems
-Related, the use of ICD-10 codes is imprecise for the diagnosis of “myocarditis” and may also include other exacerbations of underlying cardiac conditions in children with COVID-19.
(IMO the above limitations should have been a non-starter in terms of comparing post-covid to post vaccine myocarditis..
-They included MIS-C in their “cardiac complications” in this analysis but the CDC Director is not telling us MIS-C has all but disappeared as of April of 2022.

-In terms post-vaccination myocarditis, the should have had a closer-to-correct estimate of the number vaccinated (or they vaccinated denominator) but they glossed over the fact they found a rate of up to 360 cases per million of post pfizer dose 2 myocarditis. This is 1/2800 … just like Hong Kong found. The CDC was doing anything but announcing this concerning finding to the public. As most of you know, what they announce to the public is one sided- promoting vaccines and making people fear covid, so these are not mistakes. It’s intentional incorrect messaging sometimes referred to as covering up or more plainly, lying.
But what do international studies find?
The first study we had on this (originally as a preprint) was from the UK from Patone et al published in Circulation.

When one adjusts (see paper at my personal favorite preprint server Arxiv) for undiagnosed infection in the UK population, they estimate ends up being that myocarditis post dose 2 moderna was 6x higher than post COVID-19 and 1.12 x higher post pfizer dose 2 in males <40, but they did not provide stratified estimates for the highest risk group post vaccine which is the 12-24 year olds. We’ll get to that in the next study.

What did the Nordic countries, that had very high asymptomatic testing rates, find in their JAMA Cardiology study?

Well, they make this statement about post covid myocarditis rates but to compare it with post-vaccination rates, I had to go digging (Without getting anyone in trouble, I will say I have some Nordic friends and I know exactly why this information wasn’t readily apparent in the text!).

But exploring the supplements, I got what I was looking for. Focusing on myo and pericarditis combined for the full series of 2 doses and comparing it to COVID-19 for 16-24 year old males, the result is not reassuring… 6-28 x higher myo/pericarditis rates post full vaccination than post covid. The CDC is not telling you this. The question is: do they not know?
(I first reported this in October 2022 while on a flight to D.C. to give a talk with Jay Bhattacharya, Scott Atlas, Aaron Kheriaty and others)

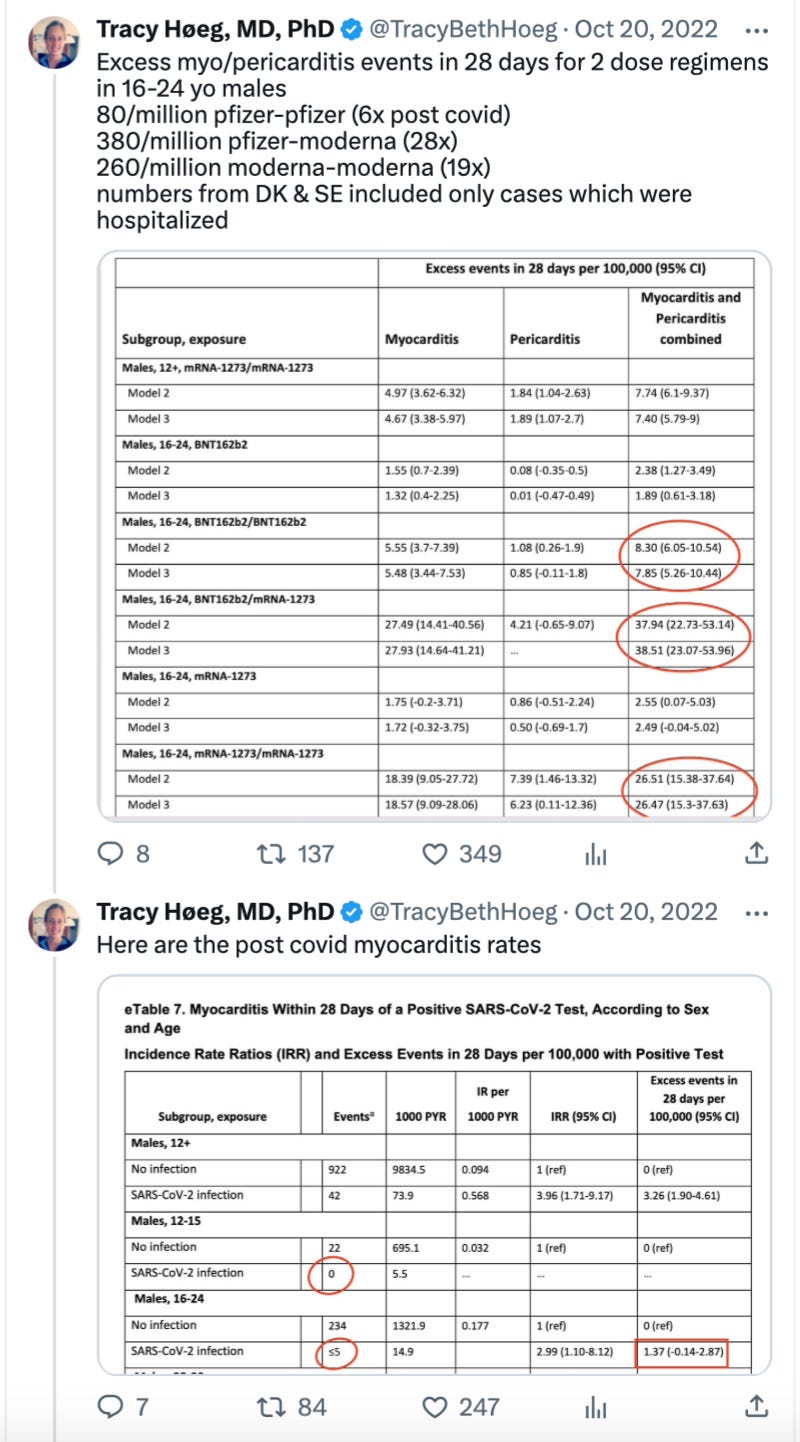
Also, look at the above carefully and note the “0” events in terms of post-covid myocarditis in males 12-15. From 4 Nordic countries with 23 million residents! Hello. Can you say rare?
Any amount of myocarditis post vaccine will be infinitely higher, according to my calculations ;-)
It also doesn’t look much better for females (though the rates of both are lower), myo/percarditis, especially if Moderna is involved, is also 7-13x higher in them post vaccination than post-Covid. Check out full details in my Twitter post and the article supplements. Note again 0 cases of post Covid myo/pericarditis in 12-15 year old females.

We are not even getting into the fact we don’t know if vaccination diminishes (or increases?) the risk of post-Covid myocarditis.
That is something Vinay Prasad, Miloš Miljković and I brought up in a letter regarding another Nordic Study here

And with multiple authors in Letter in Journal of Medical Ethics. One can’t assume vaccination benefits. One must demonstrate them with unbiased data.
Conclusion
So the CDC is misleading us, lying to us. Whatever you call it. They are wrong about post-covid-19 vs post-vaccination myo/pericarditis just like they have been wrong about natural immunity, masks, and school closures. But they show no willingness to acknowledge they were wrong or recognize the fact higher quality evidence that contradicts their findings even exists. It’s not good.
I’ll admit I do still make time to run in the mountains, but there is a lot of work left to do getting accurate public health information to the American people. To that end- what did I miss or get wrong?
