Because truth is more important than The Narrative: 10 ways the JAMA Network Open article accusing physicians of spreading misinformation is wrong
And why the "misinformation" label is antithetical to the scientific process

I recently wrote a thread on X exposing just some of the numerous obvious flaws and untruths in the recent JAMA Network Open paper . I’ve received numerous requests to do interviews and write more on this topic. I was going to write a letter to the editor based on my post but apparently JAMA NO does not accept letters to the editor.
So here I am writing on Substack, trying to get it all straight and prepare for an interview this week on the topic (I’m also secretly hoping you will let me know what I got wrong).
The JAMA NO paper’s purpose was to identify & describe (or perhaps more accurately target) physicians who the authors claimed spread “misinformation” about COVID-19.
The main problem was that the authors themselves did not actually do their research or due diligence in an attempt to to distinguish truth from falsehoods. What they did instead was refer to the CDC and “the existing state of scientific evidence” (which, as you will see, is apparently quite far from the actual truth in most instances). The authors stated:
“We defined COVID-19 misinformation as assertions unsupported by or contradicting US Centers for Disease Control and Prevention (CDC) guidance on COVID-19 prevention and treatment during the period assessed or contradicting the existing state of scientific evidence for any topics not covered by the CDC”
But let’s get to the paper’s errors in an attempt to show how labeling things “misinformation” and people as “misinformation spreaders” can so quickly go off the rails:
The first sentence of the introduction gives an inaccurate count of deaths in the United States due to COVID-19. They state, as of May 11, 2023, an estimated 1,128,000 COVID-19 deaths occurred in the US. But this is based on the flawed COVID Data Tracker which uses case report data from local health departments and not death certificates. As we showed in our study, the Data Tracker has never been accurate compared to death certificate data and is not even later corrected to align with the death certificate-base data. If you use the NCHS-based CDC Wonder, which is based on death certificates and is then able to begin to distinguish death from vs with covid by looking at underlying cause of death only, you will see, even by Monday July 17th, the number of deaths in the US due to COVID-19 was under 1 million at 980,164.

The BMJ and our research group (with Kelley Krohnert, Vinay Prasad and Alyson Haslam) have published articles describing the flaws with the COVID Data Tracker, particularly when it comes to the persistent overcounting pediatric deaths. Yet the Data Tracker is the source the authors chose to cite…
More careful adjudication of death certificates, as has been done in Finland and published in a peer-reviewed journal by Danish health authorities show 25-40% of COVID-19 deaths were incidental up through 2021 whereas starting in 2022 65-75% of deaths listed as “COVID-19” were incidental and due to other causes yet were still listed as “Covid deaths” (see Figure below). Thus the 980,000 total deaths listed as underlying cause on CDC wonder are likely still an overestimate as death certificates have not been thoroughly adjudicated in the US.

Source: Friis NU, Martin-Bertelsen T, Pedersen RK, Nielsen J, Krause TG, Andreasen V, Vestergaard LS. COVID-19 mortality attenuated during widespread Omicron transmission, Denmark, 2020 to 2022. Euro Surveill. 2023 Jan;28(3):2200547. doi: 10.2807/1560-7917.ES.2023.28.3.2200547. PMID: 36695485; PMCID: PMC9853946.
Long covid. The authors claim 14% of people “infected by the COVID-19 virus” (it’s actually the SARS-CoV-2 virus, but I’ll let this go…) have experienced post-COVID-19 condition (PCC). They cite studies which do not compare prevalence of these same symptoms in uninfected controls. This is the biggest problem with their statement. One study from Norway found PCC symptoms were equally common among infected as uninfected adolescents and young adults. This alone demonstrates how vague and poorly defined “post covid condition” is. I will be writing on this more soon.

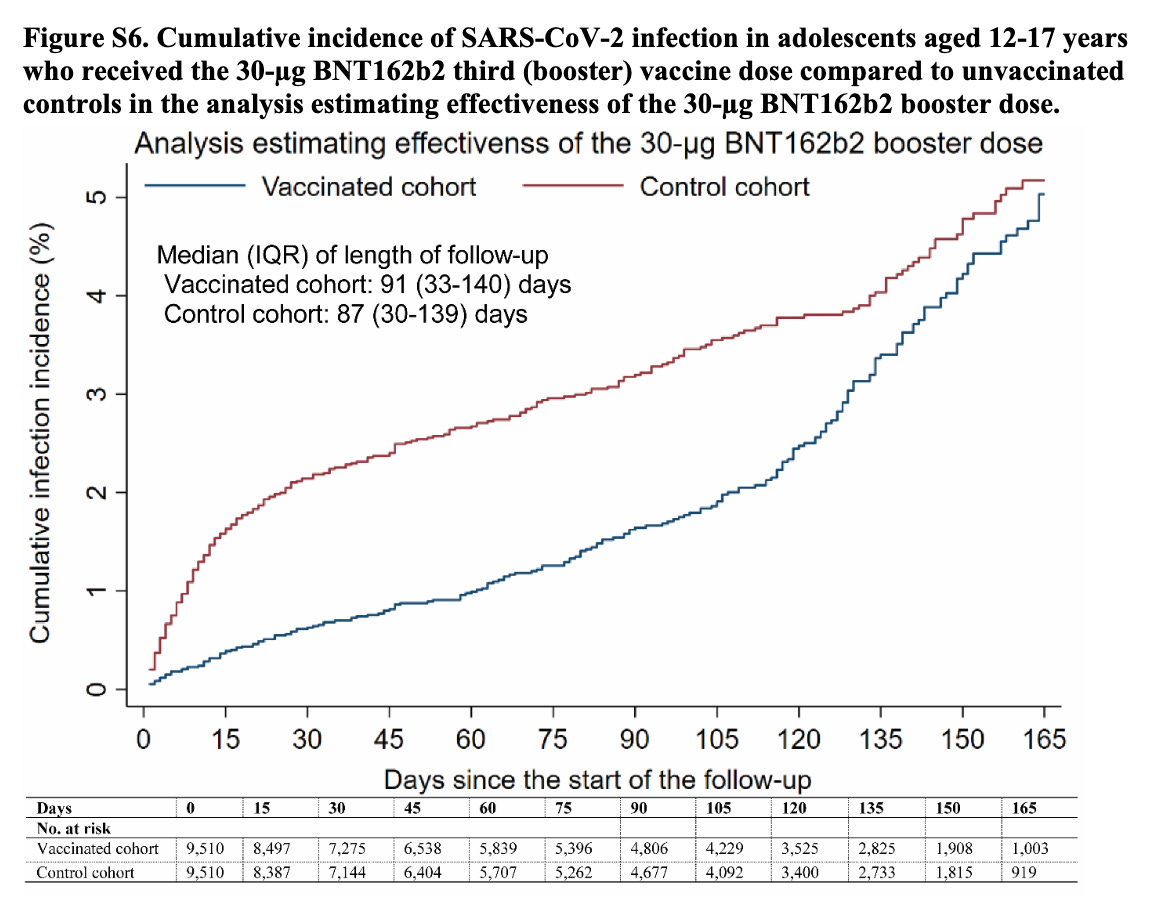
Higher death rates among unvaccinated. I'm not sure what they're citing here, but they don’t seem to be considering “healthy vaccinee bias” or, in other words, the fact that people who choose to be vaccinated may just be healthier and less likely to die than those who don’t choose vaccination which may have nothing to do with actual vaccination efficacy. This is well-described in the US… in fact, in the CDC’s own journal.
I had a recent letter published in the New England Journal with Vinay Prasad and Ram Duriseti on healthy vaccinee bias in a Clalit Health Services of Israel study of the effectiveness of the first booster against COVID-19 mortality. We found the un or later boosted had 95% higher NON covid death rate meaning, wow, they were A LOT less healthy than the boosted/early boosted. Could this explain the entire supposed 90% “effect” against COVID-19 death which the authors attributed to the booster?

Our letter is still 6th most read “article” in NEJM this past month!💥
Healthy vaccinee bias is nothing new; we’ve seen it with the Influenza vaccine year after year as well and I will be speaking to a WHO group on this topic soon!
Check out this article on healthy vaccinee bias in studies of the influenza vaccine. I absolutely love this paper by Lisa Jackson et al - healthy vaccinee bias could explain most if not all of the effectiveness against severe disease that has been attributed to the vaccine.
4. COVID vaccine ineffectiveness.

Um yes the vaccines were ineffective at preventing spread. One Danish study in Nature Communications famously showed once you were infected there was no difference in transmission rates

But prior infection does give some protection against transmission - interestingly!
SAR= secondary attack rate
And then it’s only a matter of time before the same number of vaccinated and unvaccinated people are infected as this Qatari study in NEJM showed

Hiam Chemaitelly’s group consistently does impressive work, imo. Love the above graph so much.
5. Vaccine myocarditis risks don’t exceed vaccine risks? 🤔 This sentence is just nonsense. What does this mean that "post-vaccine myocarditis risks outweigh the risks of vaccination" ? Do they mean outweigh the risks of COVID-19 that the vaccine prevents? In which case, their statement is false for previously infected adolescents. See our peer study with risk benefit analysis We found (even prior omicron), risks of post-vax myocarditis outweighed possible vax benefits after non high risk adolescent has natural immunity.

Given vaccination related cardiac death rates in adolescents and young adults appear to occur somewhere between 1 to 3/million primary series given (Korea,Qatar, UK) how could we ever say we know the vaccine benefits outweigh the risks for all kids (who even before omicron & prior immunity had a 3/million chance of death due to COVID-19)? Especially when we don’t even know how effective the vaccine is at preventing covid deaths in this group!). Saying we know the benefits of vaccination outweigh the risks for all kids regardless of prior immunity and underlying health is crazy and always has been. I was censored on Twitter for saying this June of 2021 (thanks to Tucker Carlson for featuring my post when it happened!).
6. This vax deaths "only" attributable to J&J is misleading; they are covering up international data ((Korea,Qatar, UK, Israel, Germany) from countries where better surveillance is done.

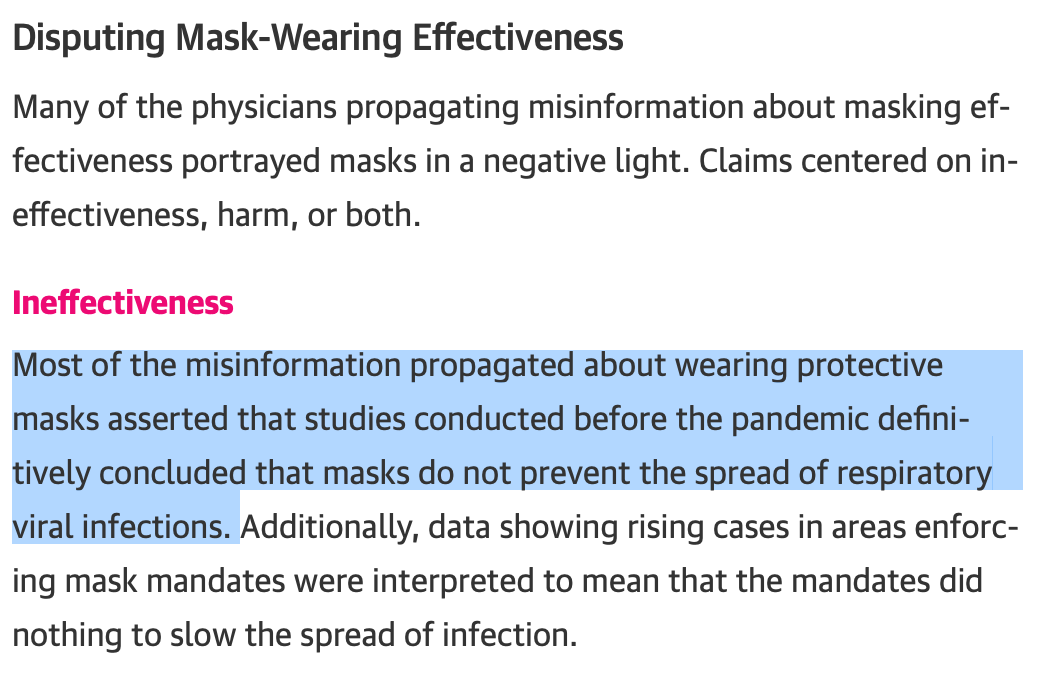
7. “Disputing mask-wearing effectiveness”. How is using randomized data on the effectiveness of masks for other respiratory viruses misinformation? Please see the Cochrane reviews of randomized studies from 2020 and updated with COVID-19 trials for 2023.
As the Cochrane review from 2023 appropriately states: “Wearing masks in the community probably makes little or no difference to the outcome of laboratory‐confirmed influenza/SARS‐CoV‐2 compared to not wearing masks”

So all of the below examples they provide of supposed “misinformation” about mask ineffectiveness are not misinformation at all.

8. This info on covid origins is also incorrectly listed as "misinformation"
This part would be hilarious if it weren't so tragic (because of how likely it is to be true). Let’s keep it simple: the presence of the furin cleavage site in SARS-CoV-2 is enough to know almost beyond a shadow of a doubt this virus is the result of gain of function research. Please see Cal Poly Microbiology Professor Pat Fidopiastis’ courses on this topic and discussion of the signature for genetic engineering in sars-CoV-2.
9. Natural immunity. Yes, the authors got this one wrong too & the anesthesiologist was right. Natural immunity is at least as good as vaccine based. This has been shown over and over and over but the best summary of evidence is published in The Lancet here.

10. Finally, a perfect note to end on is that the true statement that the US govt was colluding with tech companies to censor certain people and content regarding COVID-19, which the JAMA NO authors also (hilariously) label as “misinformation”. If you have been following the Missouri v Biden case, you know the US govt was telling social media companies to censor certain people and content because of COVID-19. This is seriously beyond silly they call this “misinformation”

———-
This act - of labeling things “misinformation”; what does it achieve? Well certainly it obscures the truth, makes people hesitant to speak up if they disagree with the consensus and is harmful to the brave doctors who are simply trying to tell the truth (and as seen here they were more correct than the CDC and the self-appointed arbiters of truth that authored and edited this article).
This “misinformation” movement, which in this case protects the government narrative, is reminiscent of Lysenkoism (a famous example of how a government’s version of The Science can result in millions of unnecessary deaths). The blacklisting of physicians is reminiscent of McCarthyism. It’s also a great example of what can go wrong when you rely on the government (in this case the CDC) rather than the current data to determine the scientific truth (and I suppose this will remind us all of Orwell and what almost happened in California under Newsom’s AB-2098). So why did the authors write it and why did JAMA NO publish it?
I suppose the authors think it will advance their career and JAMA NO wants more advertisers for and clicks to their journal? But idk you tell me. I would love to see this article retracted and a statement issued to the listed physicians (I was not one of them) that they were in fact correct- and what they wrote was not actually misinformation. But I am not holding my breath. In either case, the truth has a way of coming out eventually. But this article JAMA NO article is not making it happen any faster.